A couple came to my clinic a few years ago. 32-year-old Sonam (name changed) and her 35-year-old husband Siddharth (name changed) had been married for seven years. They had been trying to have a baby for almost six years and were found to be suffering from primary infertility.
Both of them were obese, with a BMI greater than 30 and Sonam was also suffering from hypertension. The couple was advised to reduce their weight to overcome the underlying problem. When they returned to my clinic just three months later, Sonam had lost 10 kilos. They were given some multivitamins and she conceived naturally within six months, and delivered a baby girl.
Obesity is becoming an increasingly common cause of infertility in today’s extremely fast paced world. Infertility can be defined as not being able to get pregnant even after one year of unprotected intercourse. A skewed work-life imbalance makes today’s couples opt for a sedentary lifestyle with either none or minimal physical activity. Their food habits are also erratic. They snack a lot and consume a diet of mostly fast food. This unhealthy lifestyle leads to obesity, which reduces the chances of them getting pregnant. The body mass index (BMI) of the individual determines whether one is overweight or not. One can calculate their BMI by dividing their weight in kilograms by the square of their height in meters. Having a BMI between 26 and 30 is considered to be ‘overweight’ and over 30 is considered to be ‘obese’.
Preserving Fertility in Young Cancer…
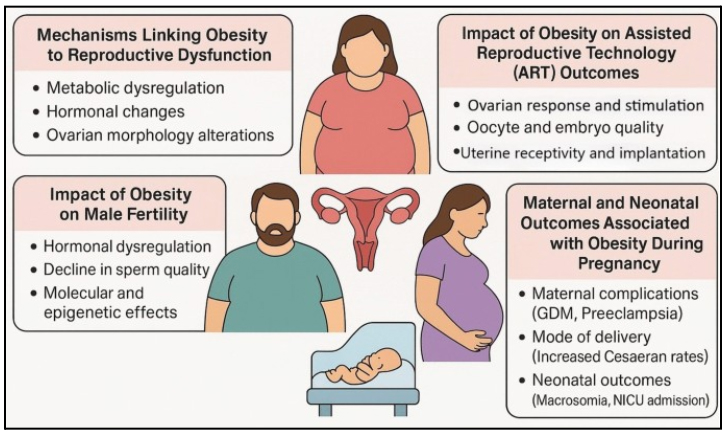
Obesity causes hormonal imbalances and problems with ovulation in women, thus affecting their ability to conceive. A large proportion of infertile women have polycystic ovary syndrome (PCOS), which is also linked to an increased risk of obesity and other metabolic anomalies. While we know that obesity is a risk factor for ovulation problems, recent research has shown that it also contributes to infertility in women who ovulate normally. In obese women, fat is deposited in the abdomen, causing the body to produce male hormones called androgens. These hormones prevent follicular maturation and contribute to anovulation (failure to release ova from ovaries). It has also been seen that the hormone leptin, which plays a major role in regulating metabolism and appetite, is also involved in the hormonal derangements related to obesity. Obesity has a substantial effect on the manifestation of polycystic ovary syndrome. Obesity is associated with infertility in men as well, resulting in decreased libido, erectile dysfunction and poor semen quality.
The worrying factor is that obesity not only makes it much more difficult to conceive, it also exposes both the mother and the infant to several risks both before and after birth. The mother faces pregnancy complications like gestational diabetes, hypertension, miscarriage, pre-eclampsia, blood clotting, infection, need for cesarean birth and stillbirth. Babies born to overweight or obese mothers are more likely than those born to mothers of healthy weight to become obese children and adults, and to have other health problems.
 For women who are obese and infertile, treating obesity should be the initial goal, before embarking on ovulation-inducing drugs or assisted reproductive techniques. The good news is that even a loss of 5-10 percent of the total body weight can significantly improve the chances of successful conception. Lifestyle modifications remain the simplest and probably the most effective solution to infertility associated with obesity. Excessive smoking and alcohol should be avoided. The couple must strive to lead a disciplined life and consume a healthy diet with less sugar, salt and fat. Two liters of water should be consumed every day along with adequate amounts of fresh fruit and vegetables. They should go for walks regularly and make it a point to exercise and be physically active. Since their overall emphasis should be on achieving and maintaining a reduced weight, it is essential for them to establish sensible eating patterns and a healthy lifestyle.
For women who are obese and infertile, treating obesity should be the initial goal, before embarking on ovulation-inducing drugs or assisted reproductive techniques. The good news is that even a loss of 5-10 percent of the total body weight can significantly improve the chances of successful conception. Lifestyle modifications remain the simplest and probably the most effective solution to infertility associated with obesity. Excessive smoking and alcohol should be avoided. The couple must strive to lead a disciplined life and consume a healthy diet with less sugar, salt and fat. Two liters of water should be consumed every day along with adequate amounts of fresh fruit and vegetables. They should go for walks regularly and make it a point to exercise and be physically active. Since their overall emphasis should be on achieving and maintaining a reduced weight, it is essential for them to establish sensible eating patterns and a healthy lifestyle.
It is important to note that obese infertile women who are above the age of 35 should not wait endlessly to lose weight before starting treatment for infertility. In case they are unable to lose weight in three to six months, even after trying hard, they should go ahead with their treatment for infertility. In an ideal situation, weight needs to be brought under control before starting any treatment for optimum results. But after the age of 35, there is a sharp decline in a woman’s ovarian reserve and egg quality becomes poor. Thus, waiting until they lose weight will only result in further deterioration of egg quality, which will reduce the chances of successful conception even more.
Weight loss improves reproductive functioning in several ways, which broadly include changes in endocrinological parameters, metabolism, fat and/or lean tissue mass and even improvements in self esteem. Initial body weight and the amount of weight lost determine the overall impact of weight loss on reproductive functioning. Obese women who lose a decent amount of weight have improved menstrual regularity, ovulation, hormonal profiles and pregnancy rates.